


Article Figures & Tables
Figures
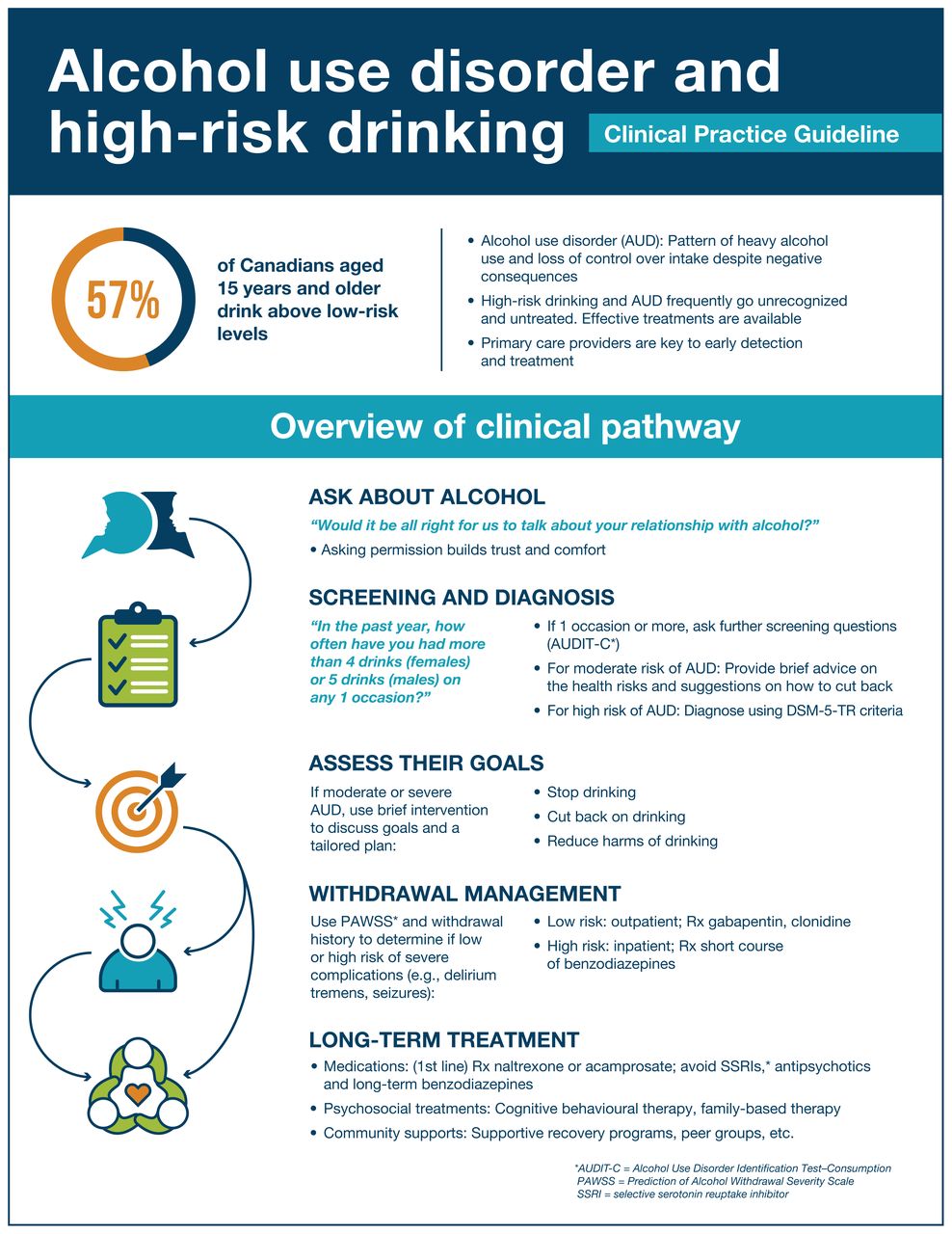
- Figure 1:
Summary of clinical pathway for alcohol use disorder. DSM-5-TR = Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision.
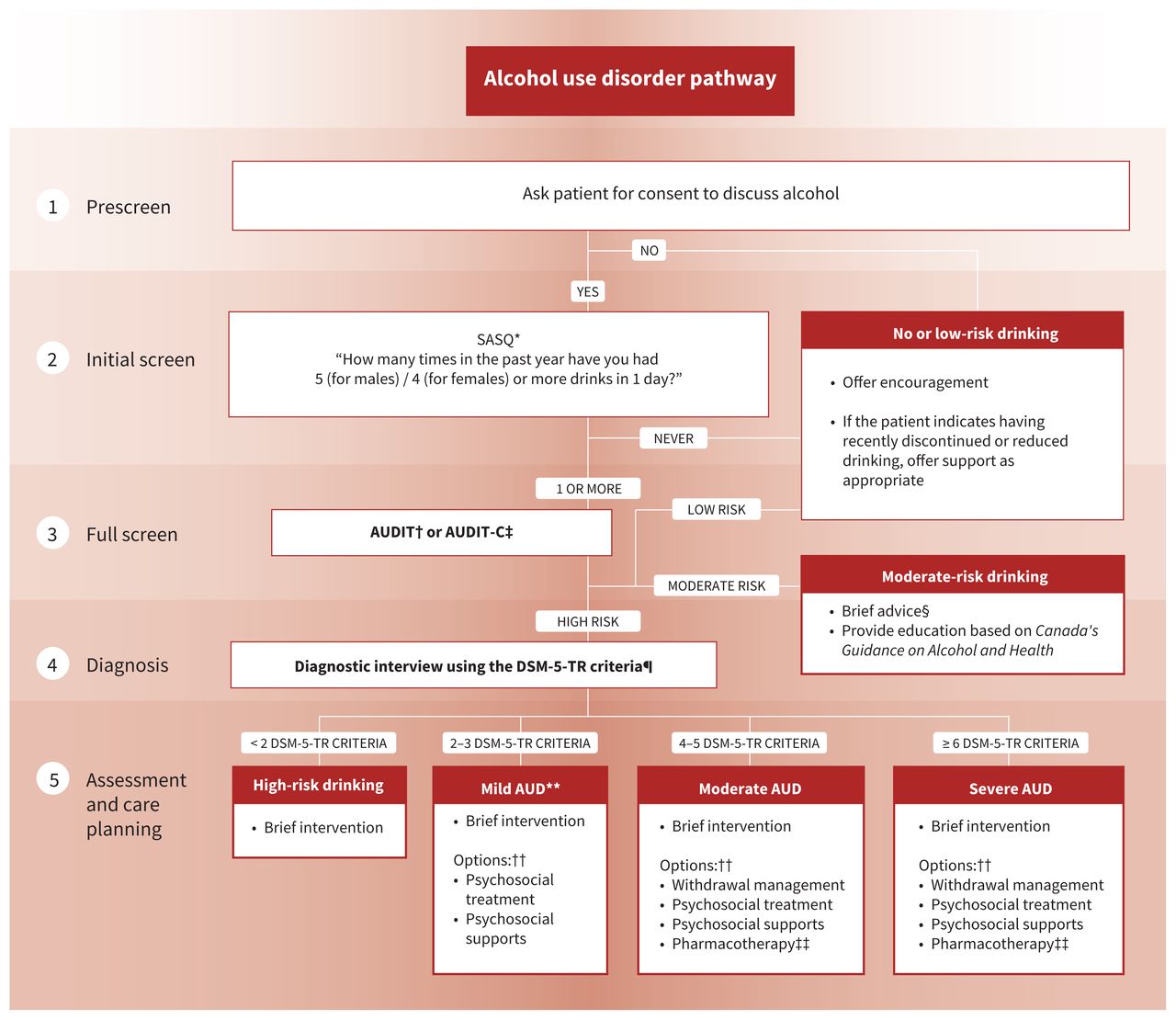
- Figure 2:
Alcohol use disorder (AUD) care pathway. Note: AUDIT = Alcohol Use Disorders Identification Test, AUDIT-C = AUDIT–Consumption, DSM-5-TR = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, SASQ = Single Alcohol Screening Question. *See Appendix 1, Section A2.2. †See Appendix 1, Box 10. ‡See Appendix 1, Box 11. §Brief advice consists of clinician-led feedback on the effects of alcohol, benefits to reducing, and strategies to reduce drinking. (2) ¶See Appendix 1, Box 5. **Previously labelled as “alcohol abuse” in DSM-IV. ††Based on patient’s goals and preferences. ‡‡First-line pharmacotherapies are naltrexone and acamprosate.
- Figure 3:
Withdrawal management pathway for alcohol use disorder. Note: AUD = alcohol use disorder, BID = twice daily, CIWA-Ar = Clinical Institute Withdrawal Assessment for Alcohol–Revised, DTs = delirium tremens, PAWSS = Prediction of Alcohol Withdrawal Severity Scale, QID = 4 times daily, SAWS = Short Alcohol Withdrawal Scale. *See Appendix 1, Box 16. †See Appendix 1, Box 7. ‡Offer oral thiamine (200 mg daily) before and during withdrawal management. In inpatient settings, offer parenteral thiamine (200–300 mg daily) for patients with suspected Wernicke encephalopathy, decompensated liver disease, or at risk of malnourishment, for 5 days minimum, followed by oral thiamine. §See Appendix 1, Box 14. ¶See Appendix 1, Box 15. **Example prescription for severe withdrawal: diazepam 10 mg BID-QID (days 1–3), 5 mg BID-QID (days 4–5), then reassess for days 6–7. Adjust daily based on symptoms and consider daily dispensing or blister packaging.

Tables
- Table 1:
Sample interview questions for DSM-5-TR criteria for diagnosis of alcohol use disorder
Diagnostic criterion* Question: “In the past year…” 1 Did you drink more or for a longer time than you had originally planned to? 2 Did you try to cut back or stop drinking, but weren’t able to? 3 Did you spend a lot of your time drinking or recovering from drinking? 4 Were you so preoccupied with wanting a drink that you found it hard to think about anything else? 5 Did you have a hard time doing your job properly or going to school because of alcohol? Taking care of your family and home? 6 Did you keep drinking even though you knew it was causing problems in your relationships? 7 Did you give up on activities or hobbies, or seeing friends because of drinking? 8 Did you get into dangerous situations more than once because of your drinking? Such as drinking and driving, unsafe sex, other situations where you could have been hurt? 9 Did you keep drinking even though it was making you feel depressed or anxious, or making a physical health problem worse? 10 Did you feel tense and anxious because it takes more drinks than it did in the past to feel intoxicated? Do you find that drinking the same amount as in the past doesn’t relieve your stress or have the same effects? 11 Did you ever have shaky hands, sweats, anxiety, hearing voices, nausea or a seizure, hours after you’d stopped drinking? Do you ever have a drink to prevent those symptoms from happening? Note: DSM-5-TR = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. (11)
↵* Refers to the numbered DSM-5-TR diagnostic criteria for alcohol use disorder. (11)
Recommendation Strength of recommendation* Certainty of evidence (15) Screening† 1 When appropriate, clinicians should inquire about current knowledge of and offer education to adult and youth patients about Canada’s Guidance on Alcohol and Health, in order to facilitate conversations about alcohol use. Strong Low 2 All adult and youth patients should be screened routinely for alcohol use above low risk.‡ Strong Moderate Diagnosis 3 All adult and youth patients who screen positive for high-risk alcohol use should undergo a diagnostic interview for AUD using the DSM-5-TR criteria§ and further assessment to inform a treatment plan, if indicated. Strong Low Brief intervention 4 All patients who screen positive for high-risk alcohol use should be offered brief intervention. Strong Moderate Withdrawal management 5 Clinicians should use clinical parameters, such as past seizures or past delirium tremens, and PAWSS (16) to assess the risk of severe alcohol withdrawal complications and determine an appropriate withdrawal management pathway. Strong Moderate 6 For patients at low risk of severe complications of alcohol withdrawal (e.g., PAWSS < 4), clinicians should consider offering nonbenzodiazepine medications, such as gabapentin, carbamazepine or clonidine for withdrawal management in an outpatient setting (e.g., primary care, virtual). Strong Moderate (gabapentin) Low (carbamazepine, clonidine) 7 For patients at high risk of severe complications of withdrawal (e.g., PAWSS ≥ 4), clinicians should offer a short-term benzodiazepine prescription, ideally in an inpatient setting (i.e., withdrawal management facility or hospital). However, where barriers to inpatient admission exist, benzodiazepine medications can be offered in outpatient settings if patients can be closely monitored. Strong High 8 All patients who complete withdrawal management should be offered ongoing AUD care. Strong Low Treatment and ongoing care Psychosocial treatment interventions 9 Adult and youth patients with mild to severe AUD should be offered information about and referrals to specialist-led psychosocial treatment interventions in the community. Strong Moderate Pharmacotherapy 10 Adult patients with moderate to severe AUD should be offered naltrexone or acamprosate as a first-line pharmacotherapy to support achievement of patient-identified treatment goals. Strong High A. Naltrexone is recommended for patients who have a treatment goal of either abstinence or a reduction in alcohol consumption. B. Acamprosate is recommended for patients who have a treatment goal of abstinence. 11 Adult patients with moderate to severe AUD who do not benefit from, have contraindications to, or express a preference for an alternate to first-line medications can be offered topiramate or gabapentin. Strong (topiramate) Moderate (topiramate) Conditional (gabapentin) Low (gabapentin) 12 Adult and youth patients should not be prescribed antipsychotics or SSRI antidepressants for the treatment of AUD. Strong Moderate 13 Prescribing SSRI antidepressants is not recommended for adult and youth patients with AUD and a concurrent anxiety or depressive disorder. Strong Moderate 14 Benzodiazepines should not be prescribed as ongoing treatment for AUD. Strong High Community-based supports 15 Adult and youth patients with mild to severe AUD should be offered information about and referrals to peer-support groups and other recovery-oriented services in the community. Strong Moderate Note: AUD = alcohol use disorder, AUDIT = Alcohol Use Disorders Identification Test, AUDIT-C = AUDIT–Consumption, DSM-5-TR = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, PAWSS = Prediction of Alcohol Withdrawal Severity Scale, SSRI = selective serotonin reuptake inhibitor.
↵* See Box 3 for details.
↵† A clinical pathway from screening to treatment is depicted in Figure 2.
↵‡ Suggested screening tests include the Single Alcohol Screening Question, (17) AUDIT (17) and AUDIT-C. (14) Other validated screening tools may be used. Routine annual screening is suggested, although there is a lack of research evidence on the optimal frequency.
↵§ See Table 1 for sample interview questions for DSM-5-TR diagnostic criteria for AUD. (11)
Characteristic First-line options Second-line options Naltrexone Acamprosate Topiramate Gabapentin Efficacy NNT to prevent return to heavy drinking is 12 (95% CI 8 to 26) (18)
NNT to prevent return to any drinking is 20 (95% CI 11 to 500) (18)
Reduced craving (Hedges’ g = 0.144 [small effect size], 95% CI 0.045 to 0.244) (19)NNT to prevent return to any drinking is 12 (95% CI 8 to 26) (18)
Increased days abstinent by 11 d (95% CI 5.08 to 16.81) (20)Decreased heavy drinking days by 9.0% (95% CI −15.3% to −2.7%) (18) Decreased drinking days by 6.5% (95% CI −12.0% to −1.0%) (18)
Increased the odds of maintaining abstinence up to 12 mo (OR 1.88, 95% CI 1.06 to 3.34) (21)Decreased % heavy drinking days (Hedges’ g = 0.5478 [medium effect size], 95% CI 0.0145 to 1.0812) (21) Concurrent alcohol use Safe to start while using alcohol, but may be more effective after withdrawal management Safe to start while using alcohol, but may be more effective after withdrawal management Safe to start while using alcohol Safe to start while using alcohol, but may be more effective if patients are abstinent for ≥ 3 d Contra-indications Naltrexone hypersensitivity
Any current opioid use (prescribed or nonmedical)
Acute opioid withdrawal
Acute hepatitis or liver failure
Acamprosate hypersensitivity
Severe renal impairment
Breastfeeding
Topiramate hypersensitivity
Pregnant or planning pregnancy
Narrow-angle glaucoma
Nephrolithiasis
Gabapentin hypersensitivity Cautions Concomitant use of valproic acid
Conditions or therapies that predispose to acidosis
Adverse effects Nausea, headache and dizziness
Starting at low dose or abstinence can reduce adverse effectsDiarrhea, vomiting and abdominal pain Psychomotor slowing, difficulty concentrating, speech or language problems, somnolence, fatigue and mood disturbance
Starting at low dose and titrating up can reduce adverse effectsAtaxia, slurred speech and drowsiness Dosing Start: 25 mg OD for 3 d
Titrate: to 50 mg OD over 2 wk as tolerated2 × 333 mg tablets TID Titrate: to 2 × 50 mg tablets BID over several weeks as tolerated Start: at 100–300 mg TID
Titrate: PRN to 1800 mg max dailyNote: BID = twice daily, CI = confidence interval, NNT = number needed to treat, OD = once daily, OR = odds ratio, PRN = as needed or when necessary, TID = 3 times daily.
↵* There are limited data to support combination pharmacotherapy. Single-medication trials are suggested at first. Suggested duration is 6 months or longer. We gathered information for contraindications, cautions, adverse effects and dosage from the cited clinical trials and Health Canada–approved product monographs.
↵† Safety and efficacy have not been well established in these patient populations. Careful assessment of benefit and risks, fully informed patient consent and more frequent monitoring are advised.
- Table 4:
Other national and selected international guidelines considering alcohol use, high-risk drinking and alcohol use disorder published in the last 5 years
Organization and guideline title Year Country Summary Key differences with our guideline Canadian Centre on Substance Use and Addiction: Canada’s Guidance on Alcohol and Health (2) 2023 Canada This guidance is based on the latest research on alcohol-related risks and replaces Canada’s Low-Risk Alcohol Drinking Guidelines issued in 2011. Our guideline provides recommendations on the full treatment pathway, including screening, diagnosis, withdrawal management and ongoing treatment. American Psychiatric Association: Practice Guideline for the Pharmacological Treatment of Patients with Alcohol Use Disorder (56) 2018 United States This guideline focuses on pharmacologic treatments for AUD, but also includes statements related to AUD assessment and treatment planning. Our guideline provides recommendations on the full treatment pathway and updated pharmacotherapy strategies, including off-label medications with and without proven benefit, as well as polypharmacy concerns and medications to avoid. American Society of Addiction Medicine: The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management (57) 2020 United States This guideline provides updated information on evidence-based strategies and standards of care for alcohol withdrawal management in both ambulatory and inpatient settings. Our guideline provides recommendations on the full treatment pathway, including screening, diagnosis, withdrawal management and ongoing treatment. Australian Government: The Guidelines for the Treatment of Alcohol Problems (58) 2021 Australia This is the fourth edition of a guideline for primary care and specialists, with evidence-based recommendations for screening, brief intervention, withdrawal management, psychosocial interventions and pharmacotherapies. It includes chapters for youth, gender-specific issues, pregnant and breastfeeding populations, older adults, Indigenous Peoples and other diverse populations. Our guideline provides updated pharmacotherapy strategies, including medications to avoid. Australian Government and the National Health and Medical Research Council: Australian Guidelines to Reduce Health Risks from Drinking Alcohol (59) 2020 Australia This guideline focuses on recommendations for reducing the health risks associated with drinking alcohol for adults, pregnant and breastfeeding people and people younger than 18 yr. Our guideline provides recommendations on the full treatment pathway, including screening, diagnosis, withdrawal management and ongoing treatment. Canadian Coalition for Seniors’ Mental Health: Canadian Guidelines on Alcohol Use Disorder Among Older Adults (60) 2019 Canada This guideline provides guidance for clinicians on preventing, screening, assessing and treating AUD among older individuals (aged ≥ 65 yr). Our guideline contains guidance for youth (aged 11–25 yr) and adult populations. Our guideline does not include recommendations on prevention of AUD. Our guideline includes updated guidance from Canada’s Guidance on Alcohol and Health. Note: AUD = alcohol use disorder.
In this issue

Article tools






{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Harms and costs of proposed changes in how alcohol is sold in Ontario
- Addressing the risks of antidepressants among people with alcohol use disorders
- Navigating the nuances of the Canadian guidelines stance on selective serotonin reuptake inhibitors in concurrent alcohol use disorder and mood or anxiety disorders
- Concerns regarding the recommendation against prescribing selective serotonin reuptake inhibitors in the Canadian guideline for the clinical management of high-risk drinking and alcohol use disorder
- Trouble grave lie a lutilisation dalcool apres linstauration dun traitement par inhibiteur selectif du recaptage de la serotonine
- Severe alcohol use disorder after initiation of selective serotonin reuptake inhibitor therapy
More in this TOC Section
Similar Articles
Collections


Podcast