


- © 2007 Canadian Medical Association
As the influenza season winds to a close in the southern hemisphere, public health programs in Canada are preparing to launch vaccination campaigns to protect against an infection that accounts for about 4000 excess deaths each winter.1 The number of reported cases of influenza is 3 times greater than average in several Australian states as of September 2007; however, the influenza strains in circulation are similar to those that were seen in the 2006/07 season in the northern hemisphere, and they match well with the strains covered by the seasonal vaccine.2 In Canada, the recommendations for influenza prevention are revised yearly by the National Advisory Committee on Immunization in response to updated surveillance and laboratory and clinical evidence. In this Public Health column, 2 important changes in the recommendations for the 2007/08 season are highlighted (Box 1, Box 2).3 Vaccination against influenza is now recommended for all pregnant woman, and the recommended vaccination schedule for children aged 9 years or younger has been changed. The committee has also reiterated the importance of vaccination as the primary means of preventing influenza.

It is recognized that pregnant women with concurrent conditions, such as cardiac or pulmonary disease, are at high risk for complicated influenza.4 However, the rate of immunization among pregnant women is low.5 Recently, 2 Canadian studies have shown that healthy pregnant women with influenza are more likely than nonpregnant women with influenza to have medical visits and to be admitted to hospital.6,7 Theoretically, expanding immunization programs to include all pregnant women may increase immunization uptake among pregnant women at high risk for complicated influenza. The provision of a universal program for influenza vaccination in Ontario has been associated with an increase in the rate of vaccination coverage among people with chronic conditions to 56% from 38% between 1996 and 2001. In all other provinces combined, the immunization rate increased to 38% from 27% between 1996 and 2001.8 A strategic approach to capturing this changing population will need to be considered by primary care practitioners, specialists providing obstetric care and public health.5
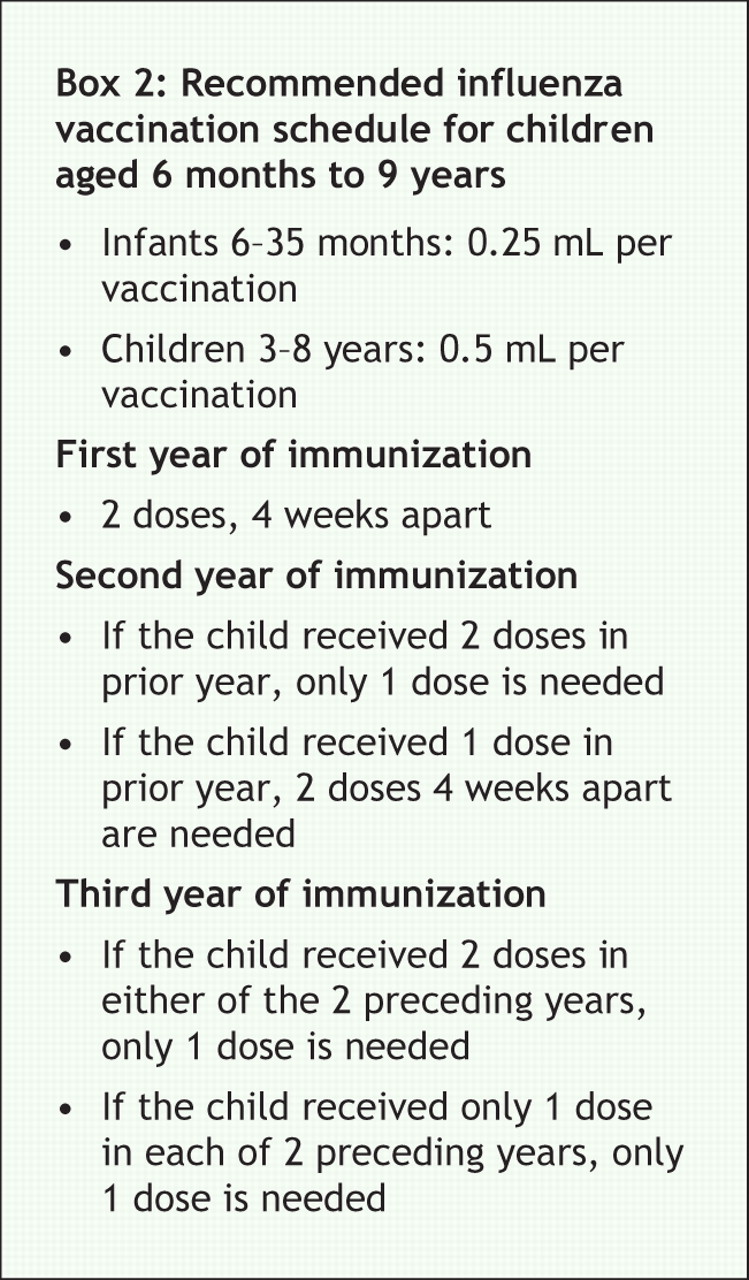
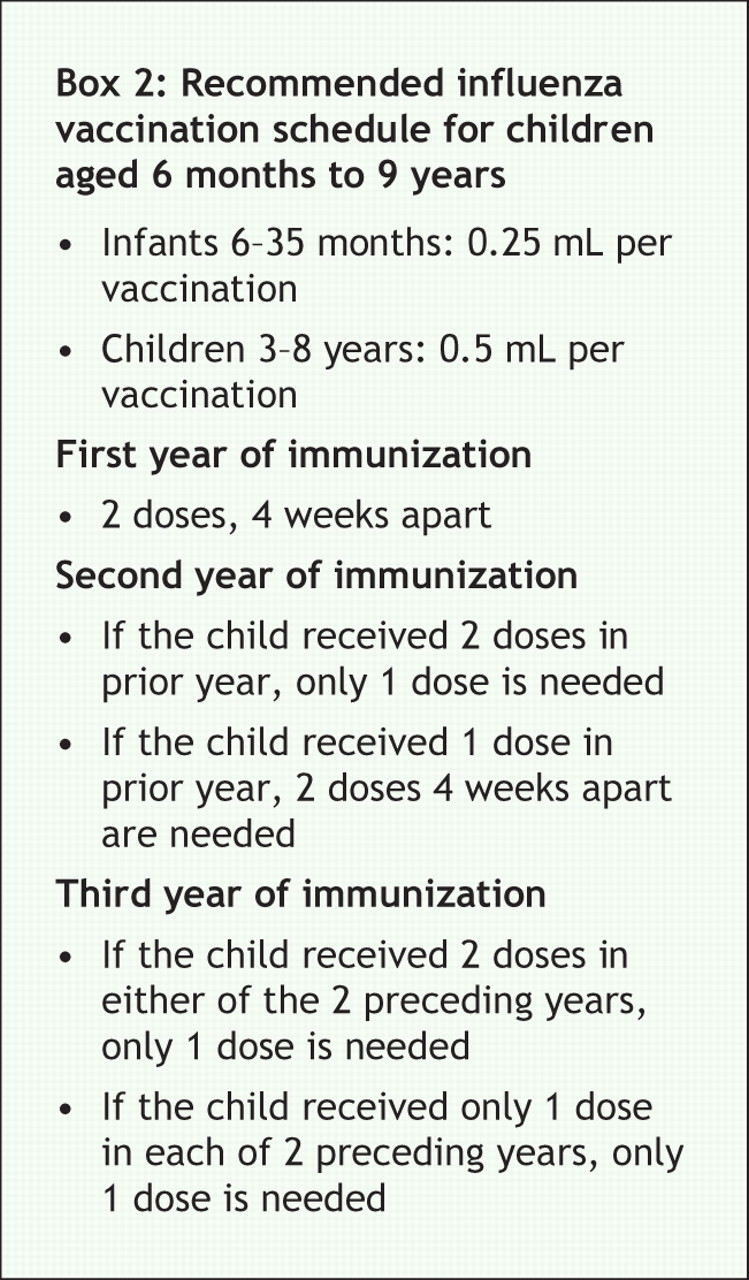
The second major change in the recommendations involves children under 9 years of age who received only 1 dose of vaccine in the previous year. A single dose of vaccine in the first year of vaccination does not appear to provide protection.9–11The committee now recommends a 2-dose schedule for children under 9 years of age if they received only 1 dose in the previous year (Box 2). This recommendation is based on evidence of reduced protection against influenza among children who received only 1 dose in their first and second years of vaccination. This recommendation parallels those made by the American Academy of Pediatrics and the Advisory Committee on Immunization in the United States.3,12
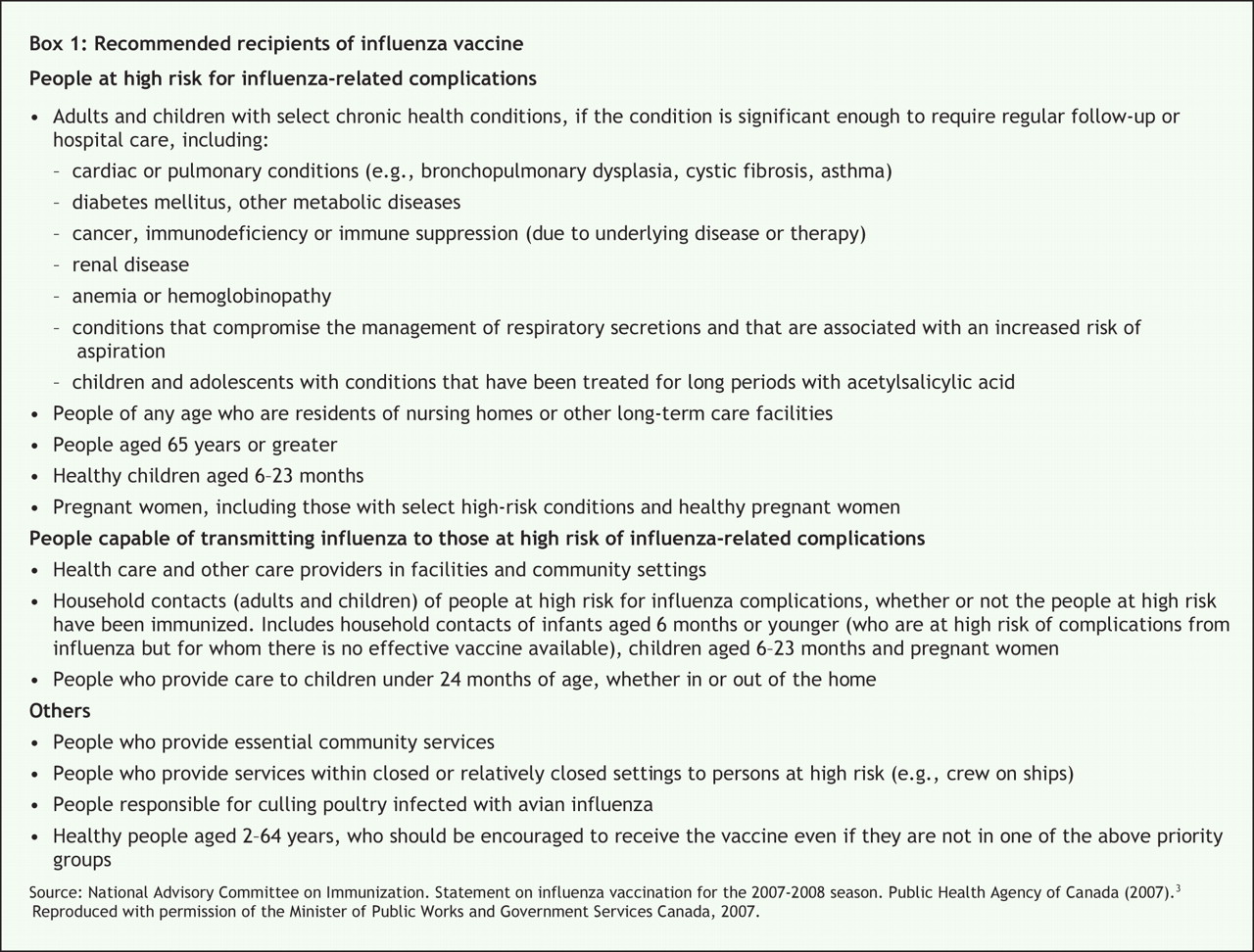
Other major recommendations from the National Advisory Committee on Immunization have not changed. They strongly recommend immunization for people who are considered at high risk for complications from influenza (Box 1). Vaccination of people who may transmit influenza to those at high risk, such as caregivers or household members, continues to be a key recommendation to prevent influenza-related morbidity and mortality (Box 1). The committee also continues to encourage vaccination for personal protection against influenza (i.e., direct benefit) for people aged 24 months–64 years who are not pregnant, are healthy and who will not be in close contact with people at high risk. The potential indirect benefit of vaccination among healthy people for the prevention of the secondary spread of influenza continues to be a focus of research and topic of discussion in the public health community.13
As in 2006/07, the National Advisory Committee on Immunization recommends that only neuraminidase inhibitors, not amantadine, be used for antiviral prophylaxis. Antiviral prophylaxis is most likely to be used in short-or long-term care institutions, including residential settings, where influenza outbreaks occur, or for people who are at high risk but cannot be vaccinated or who may have an inadequate immune response (e.g., people who are immune compromised). This recommendation was made in late 2006 when antiviral-susceptibility testing revealed that most isolates were resistant to amantadine and that these drug-resistant viruses were present throughout Canada. Although the prevalence of resistant strains in 2006/07 was lower than in the previous season, the continued presence of amantadine-resistant strains of influenza means that amantadine cannot be used to provide protection for vulnerable people. Randomized controlled trials of neuraminidase inhibitors as seasonal prophylaxis or as postexposure prophylaxis indicate these drugs are 56%–90% effective in preventing laboratory-confirmed influenza among healthy people.14 The National Advisory Committee on Immunization notes that antiviral prophylaxis should be considered only as an adjunct to immunization for influenza prevention.
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

