


A 50-year-old male farmer, a chronic smoker (30 pack-years), was referred to our Institute for persisting pulmonary opacity in chest radiographs taken over an 12-year period. He had chronic cough and mild dyspnea upon exertion. His stature was short (height 145 cm). Around his knee and wrist joints he had several painless, bony protruberances, first noticed during childhood. He was able to recount a family history of similar bony swellings involving 5 generations (Fig. 1).
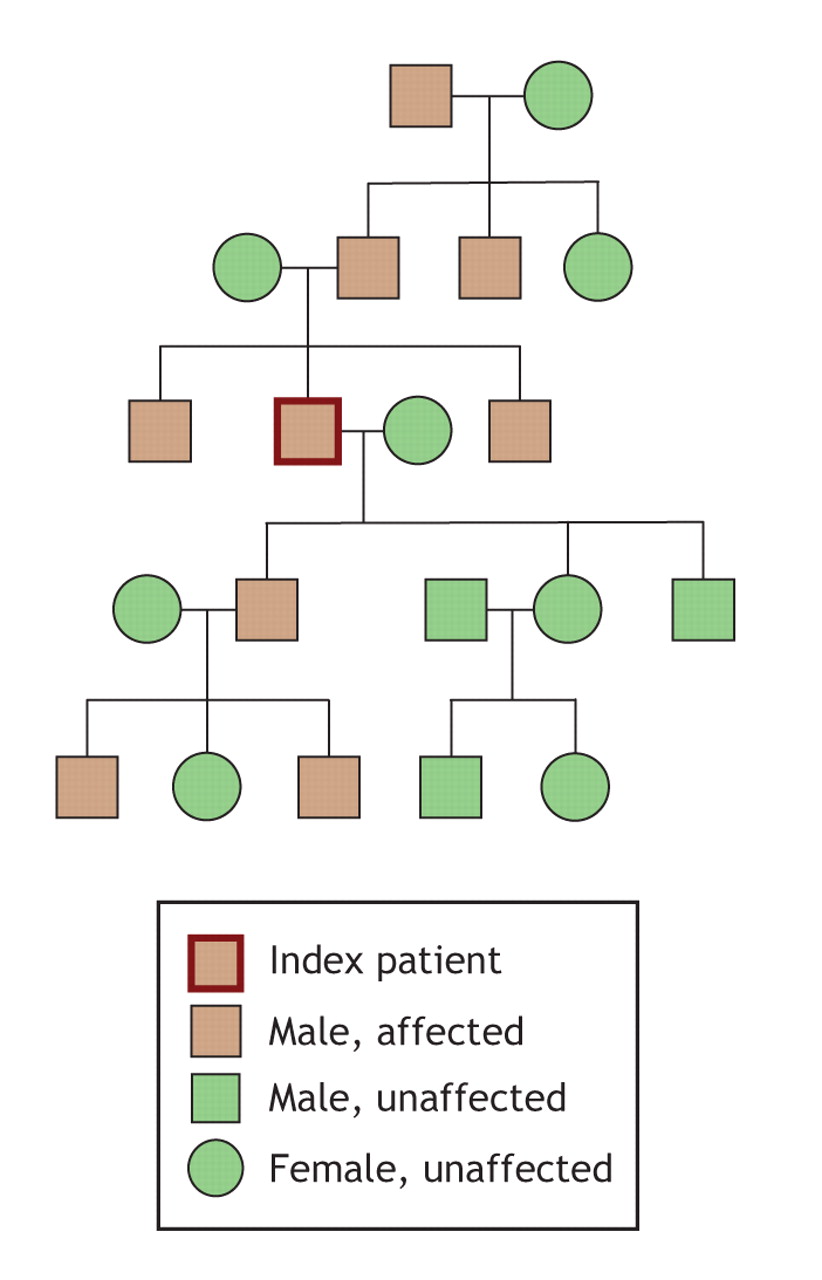
Fig. 1: Pedigree of the patient's affected family members (brown boxes; those not affected are shown in green).
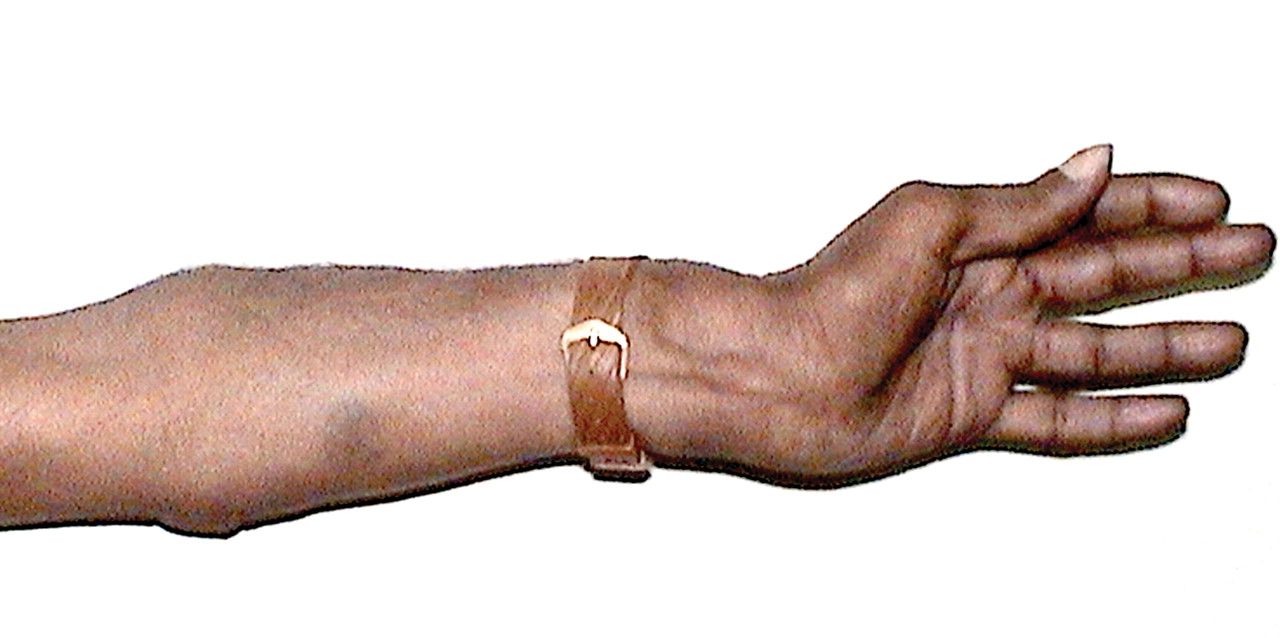
Examination revealed the bony outgrowths around the knee joints to be fixed and bilateral, with a mild genu valgum on the left side (Fig. 2). His left forearm had an had ulnar deviation (Fig. 3). Movement of his shoulders, hips and knees was within the normal range and without neurovascular problems. His chest radiograph showed a lesion of fourth left rib as a rounded, heterogeneous opacity (Fig. 4); a CT scan of the thorax confirmed the lesion to be an exostosis of fourth left rib. Radiographs of the patient's joints showed multiple bony exostoses around the knee (Fig. 5) and a lesion at the lower end of his left ulna (Fig. 6). On the basis of these clinical findings, we made a diagnosis of hereditary multiple exostoses (HME).

Fig. 2: Photograph of the patient's knees, showing bilateral bony outgrowths around both joints and a genu valgum on the left leg only.

Fig. 3: Ulnar deviation of the patient's left forearm.

Fig. 4: Chest radiograph (left) and CT scan revealing a persistent lesion (exostosis) on the patient's left fourth rib.

Fig. 5: Radiograph of the knee region; bilateral bony outgrowths are evident.

Fig. 6: Radiograph of the patient's wrists. Note the lesion at the lower end of the left ulna.
HME is characterized by multiple exostoses: benign cartilage-capped bone tumours that grow outward from the metaphyses of the long bones. Reported prevalences of HME vary widely, from as high as 1% of a small population in Guam to 1 case in 100 000 in European populations. In the state of Washington, the prevalence has been estimated to be around 1 in 50 000.1
Family histories of patients with HME suggest an autosomal dominant inheritance pattern, with a penetrance of around 96% (sporadic cases of non-penetrance have occurred among women). Linkage studies have identified 3 chromosomal locations: the EXT1 gene (chromosome 8, locus 8q24.1), EXT2 (chromosome 11, in the pericentric region) and EXT3 (chromosome 19, locus 19p). In affected families, 56%–78% have mutations affecting the EXT1 gene; 21%–44%, affecting EXT2; and a very small minority, EXT3.2 EXT genes appear to act to suppress tumours.
The initiation of tumour development may follow a multistep model. Exostoses grow and gradually ossify during skeletal development, then stop growing with skeletal maturity. The proportion of individuals with HME who have clinical findings increases from about 5% at birth to 96% at 12 years of age,1 with a median age at diagnosis of 3 years. The number of exostoses in an affected person varies widely, even within families. Involvement is usually symmetric. Various features associated with exostoses are presented in Box 1.

Sarcomatous degeneration of an exostosis is potentially life-threatening, and constitutes the most serious complication of HME. The signs of sarcomatous transformation, especially in a physically mature person, include rapid growth, increasing pain and/or neurologic symptoms.3
In asymptomatic subjects, exostoses require no therapy. Surgery is often required, however, to treat angular deformities; pain caused by irritation of skin, tendons or nerves; and leg-length inequalities.1
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

