


- © 2007 Canadian Medical Association
Abstract
Background: Many Canadian patients who receive hemodialysis live far from their attending nephrologist, which may affect clinical outcomes. We investigated whether patients receiving hemodialysis who live farther from their attending nephrologist are more likely to die than those who live closer.
Methods: We studied a random sample of 18 722 patients who began hemodialysis between 1990 and 2000 in Canada. We calculated the distance between each patient's residence location at the start of dialysis and the practice location of their attending nephrologist. We used Cox proportional hazards models to examine the adjusted relation between distance and clinical outcomes (death from all causes, infectious causes and cardiovascular causes) over a follow-up period of up to 14 years.
Results: During the follow-up period (median 2.5 yr, interquartile range 1.0–4.7 yr), 11 582 (62%) patients died. Compared with patients who lived within 50 km of their nephrologist, the adjusted hazard ratio of death among those who lived 50.1–150 km away was 1.06 (95% confidence interval [CI] 1.01–1.12), 1.13 (95% CI 1.04–1.22) for those who lived 150.1–300 km away and 1.13 (95% CI 1.03–1.24) for those who lived more than 300 km from their nephrologist (p for trend < 0.001). The risk of death from infectious causes increased with greater distance from the attending nephrologist (p for trend < 0.001). The risk of death from cardiovascular causes did not increase with distance from the attending nephrologist (p for trend = 0.21). Compared with patients who lived within 50 km of their nephrologist, the adjusted hazard ratio of death among those who lived more than 300 km away was 1.75 (95% CI 1.32–2.32) for infectious causes and 0.93 (95% CI 0.79–1.09) for cardiovascular causes.
Conclusions: Mortality associated with hemodialysis was greater among patients who lived farther from their attending nephrologist, as compared with those who lived closer. This was especially evident for death from infectious causes.
In Canada, no one is denied renal replacement therapy because of their residence location; however, a substantial proportion of patients receiving dialysis live more than 300 km from the closest nephrologist.1 Since this geographic barrier may make it more difficult to provide high-quality renal care, it is plausible that disparities in access to appropriate care may result in differences in health outcomes. Despite the potential implications for health policy, this issue has not been formally studied.
We sought to examine this issue using data collected prospectively from patients who began hemodialysis in Canada between 1990 and 2000. We hypothesized that patients who lived farther away from their attending nephrologist would be more likely than patients who lived closer to die after starting dialysis.
Methods
Study population and data sources
We conducted this study using data from the Canadian Organ Replacement Register.2,3 Data are reported to the registry by all dialysis providers in Canada and include demographic, clinical and outcome data that are collected by use of a standardized instrument. The registry has been used to conduct multiple clinical studies involving patients with kidney failure; however, it has never been formally validated.
We analyzed data from a random 75% sample of all patients who began dialysis in Canada between Jan. 1, 1990, and Dec. 31, 2000. Detailed methods are available online (Appendix 1, www.cmaj.ca/cgi/content/full/177/9/1039/DC2). We calculated the distance between each patient's residence location and the practice location of their attending nephrologist. We hypothesized a priori that the relation between distance and mortality may vary by dialytic modality; thus, we restricted our analysis to data from patients receiving hemodialysis. Our findings related to peritoneal dialysis, including outcomes specific to this therapy (e.g., technique failure), have previously been reported.4
This study was approved by the health research ethics board at the University of Alberta.
Exposures
Both the local physician supply and the socioeconomic attributes of a patient's residence location may influence their access to health care;5 thus, we assessed these characteristics for defined geographic regions. The Canadian census reports data in geographic units termed census consolidated subdivisions, which constitute municipalities or their equivalents. We used data from the Southam Medical Database to determine the population to physician ratio in each subdivision during the year that dialysis was initiated for each patient.6 The population to physician ratio was calculated separately for primary care physicians and for specialists. We estimated socioeconomic status for participants using the neighbourhood income per person equivalent, which is a household size-adjusted measure of household income.7
We used ArcGIS software (version 9.1, ESRI) to determine the shortest distance by road between each patient's residence at the time dialysis was started and the practice location of their attending nephrologist.8–10 We also classified residence location into the following regions:1 British Columbia (includes the Yukon Territory), Alberta (includes the Northwest Territories), Saskatchewan, Manitoba (includes Nunavut), Ontario, Quebec and the Atlantic provinces (includes New Brunswick, Nova Scotia, Prince Edward Island, and Newfoundland and Labrador).
Outcomes
The primary outcome was mortality from all causes. We performed secondary analyses in which we subdivided cause of death as infectious, cardiovascular or other. These subgroups were based on the cause of death listed in the Canadian Organ Replacement Register. In all analyses, follow-up was censored at loss to follow-up, renal transplantation or at the end of study.
We investigated the association between distance from the patient's residence to the attending nephrologist and the clinical outcomes. We arbitrarily categorized driving distance as follows: 0–50 km, 50.1–150 km, 150.1–300 km and more than 300 km. These categories were defined a priori. We categorized driving time as 0–30 minutes, 31–90 minutes, 91–180 minutes and more than 180 minutes.
Statistical analyses
We adjusted Cox proportional hazards models for age; sex; ethnic background (white, Aboriginal or other); cause of end-stage renal disease (diabetic nephropathy, glomerulonephritis, hypertensive or ischemic renal disease, polycystic kidney disease and other); year of dialysis initiation; comorbidities (diabetes mellitus, coronary disease, hypertension, current heart failure, stroke or transient ischemic attack, chronic lung disease, peripheral vascular disease and malignant disease); smoking status; and neighbourhood socioeconomic status. We also adjusted for geographic region and residence location. We determined that the proportional hazard assumption was satisfied by examining plots of the log-negative-log of the within-group survivorship probabilities versus log-time. We tested the robustness of our findings by performing a variety of sensitivity analyses (Appendix 1, available online at www.cmaj.ca/cgi/content/full/177/9/1039/DC2).
Demographic and clinical characteristics were described by use of counts and percentages for categorical variables, and by use of medians and interquartile ranges for continuous variables. Additionally, we used the χ2 and the Kruskal–Wallis tests where appropriate.
Results
Patient characteristics
We identified 26 808 patients aged 18 years or older who began dialysis between Jan. 1, 1990, and Dec. 31, 2000. Of these, 18 722 (69.8%) received hemodialysis and were included in our study. At the start of dialysis, 13 818 (74%) of patients lived within 50 km of their attending nephrologist, 1235 (6.6%) lived within 150.1–300 km and 882 (4.7%) lived more than 300 km away from their nephrologist. Patients who lived farther away were more likely than those who lived closer to be Aboriginal, to be younger, to have diabetic nephropathy as the cause of end-stage renal disease and to live in a lower-income neighbourhood (Table 1). Patients who resided farther from their nephrologist were healthier, since coronary disease, prior stroke or transient ischemic attack and peripheral vascular disease were less common among these patients, as compared with patient who lived in an urban residence location.
Table 1.
All-cause death
The median follow-up period was 2.5 years (interquartile range 1.0–4.7 years). During this period, 11 582 (61.8%) patients died. Mortality was significantly higher among patients who lived farther from their nephrologist, compared with those who lived closer. The adjusted rate of death per 100 person-years was 13.0 (95% confidence interval [CI] 12.1–13.9) for those who lived within 50 km of their nephrologist, 13.8 (95% CI 12.7–14.9) for those who lived within 50.1–150 km, 14.5 (95% CI 13.1–16.0) for those who lived within 150.1–300 km and 14.7 (95% CI 13.2–16.4) for those who lived more than 300 km from their nephrologist (p for trend < 0.001). Compared with patients who lived within 50 km of their nephrologist, the adjusted hazard ratio of death was 1.06 (95% CI 1.01–1.12) for those who lived within 50.1–150 or 150.0–300 km and 1.13 (95% CI 1.04–1.22) for those who lived more than 300 km away (p for trend < 0.001) (Figure 1, Appendix 2 [available online at www.cmaj.ca/cgi/content/full/177/9/1039/DC2]). The results were similar when we repeated the analyses using the 7 category classification of distance and when we performed the analyses using driving time instead of distance (data not shown). Adjustment for physician supply did not influence our results, which suggests that reduced access to local primary care physicians or non-nephrologist specialists was not responsible for the increased risk of death among people who lived far from their nephrologist.
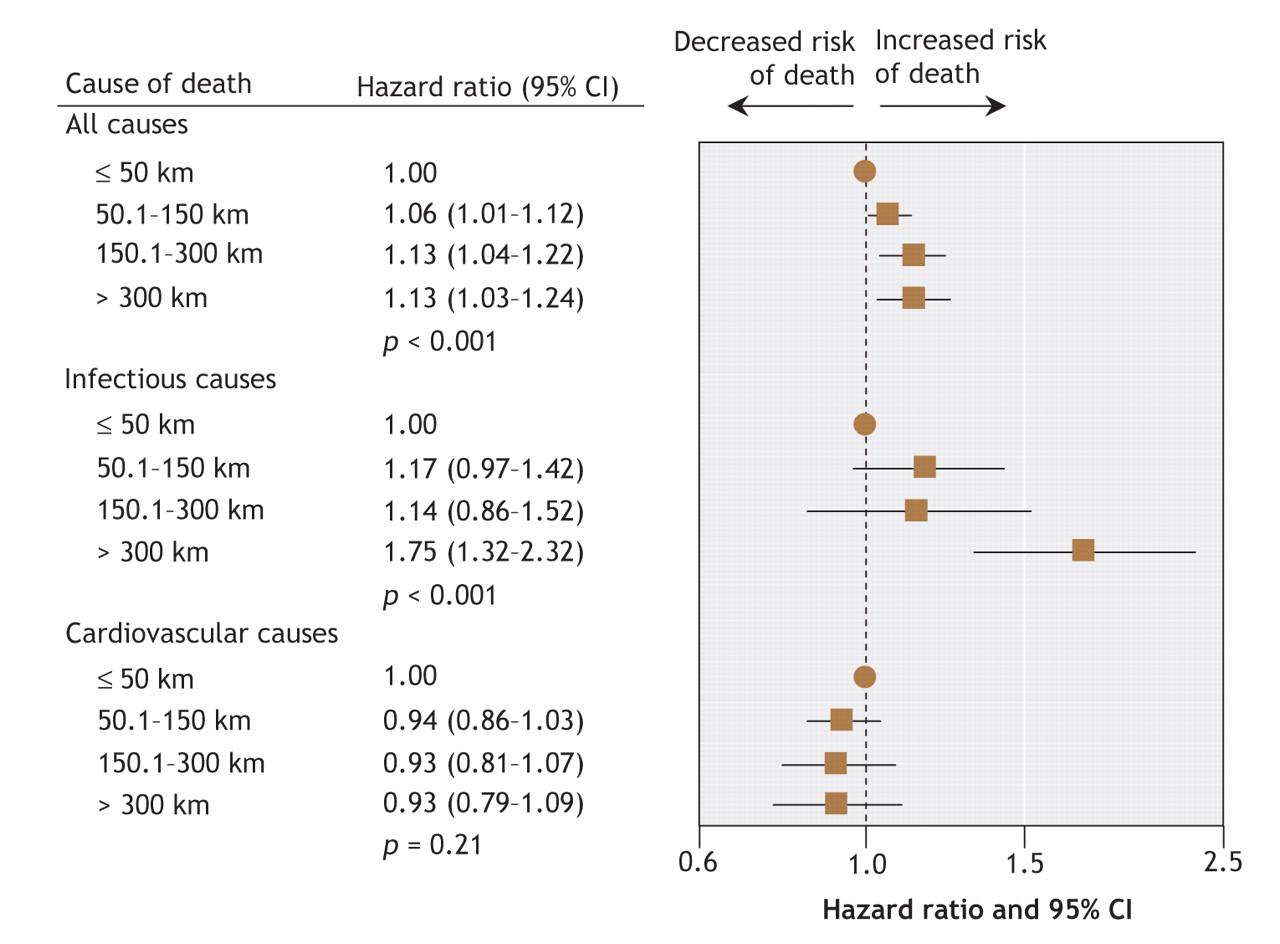
Figure 1: Forest plot showing the risk of mortality among patients receiving hemodialysis, by distance to the attending nephrologist. CI = confidence interval.
Deaths due to infectious causes or cardiovascular disease
Of 11 582 deaths during the study period, 832 (7.2%) were from infection, 4115 (35.5%) were from cardiovascular causes and 4301 (37.1%) were because of other causes. In the latter category, 1924 (16.6%) deaths were due to withdrawal from dialysis, 594 (5.1%) were from malignant disease and 214 (1.8%) were from hemorrhage. The remaining deaths were due to miscellaneous (1569 [13.5%]) or unknown (2334 [20.2%]) causes. The frequency of missing information for cause of death was similar across the 4 distance categories (p = 0.26 by χ2). When we stratified the results by cause of death, the risk of death from infectious causes increased with greater distance from the attending nephrologist (p for trend < 0.001). The risk of death from cardiovascular causes did not increase with distance (p for trend = 0.21). Compared with patients who lived within 50 km of their attending nephrologist, the hazard ratio for infectious disease among patients who lived more than 300 km from their nephrologist was 1.75 (95% CI 1.32–2.32). For cardiovascular death, the hazard ratio was 0.93 (95% CI 0.79–1.09) for patients who lived more than 300 km from their nephrologist (Figure 1, Appendix 2 [available online at www.cmaj.ca/cgi/content/full/177/9/1039/DC2]).
When we analyzed the data using distance to the attending nephrologist as a continuous linear variable, we obtained the following hazard ratios for every 100 km: 1.03 (95% CI 1.02–1.05, p < 0.001) for all-cause death, 1.12 (95% CI 1.07–1.18, p < 0.001) for death from infectious causes and 0.98 (95% CI 0.95–1.01, p = 0.15) for death from cardiovascular causes.
Subgroup analyses
We tested for 2-way interactions between age, sex, ethnic background, diabetic status and socioeconomic status on the relation between distance from the attending nephrologist and the risk of death from all causes. None of these interactions were statistically significant, which suggests that the increased likelihood of death observed among patients who lived farther away from their nephrologist was not influenced by these characteristics. Results were generally consistent when we stratified the analyses by geographic region. There was an increased risk of death among patients who lived more than 300 km from the attending nephrologist in 6 of 7 regions, with the exception being patients in Saskatchewan (p for interaction = 0.04). The adjusted hazard ratio of death was 0.83 (95% CI 0.64–1.06) among Saskatchewan residents who lived 50.1–150 km from the attending nephrologist, 0.98 (95% CI 0.77–1.26) among patients who lived 150.1–300 km away and 1.04 (95% CI 0.70–1.54) for those who lived more than 300 km away (p for trend = 0.78).
Sensitivity analyses
To address the possibility that missing information about comorbidities may have affected our results, we performed additional analyses that excluded participants with missing comorbidity data. Similarly, we assessed the potential impact of missing information about ethnic background by assuming that all people missing these data were white or Aboriginal. We performed a third sensitivity analysis that examined the effect of ethnic background by including only white patients, which did not influence our findings. The results were similar for each of these analyses, which suggests that both missing data and the restriction of the study population to hemodialysis patients were unlikely to have affected our conclusions. The results were also similar when we used distance to the closest hemodialysis unit, rather than distance to the attending nephrologist, to classify residence location (data not shown).
Interpretation
In Canada, most patients live within 50 km of their nephrologist at the start of hemodialysis; however, we found that a substantial proportion (12%) lived more than 150 km away. This distance may be a barrier to the provision of high-quality care. We found an increased risk of death after hemodialysis initiation among patients who lived in remote areas, which was particularly evident for death from infectious causes. Furthermore, the risk of death increased with distance from the attending nephrologist, and we consistently observed higher mortality among patients who live in remote areas for a variety of subgroup and sensitivity analyses.
The excess risk of all-cause death among patients who lived more than 300 km from their nephrologist was modest when expressed in relative terms (about a 13% increase compared with those who lived within 50 km). However, when expressed as absolute risk, there is a substantial increase (1.7 excess deaths per 100 person-years) owing to the high mortality associated with kidney failure. This risk is about 3-times greater than the excess risk of death associated with diabetes mellitus in the general population (0.54 excess deaths per 100 person-years, as compared with patients without diabetes).11 Thus, living in a remote area appears to be a clinically relevant risk factor for mortality among patients receiving hemodialysis in Canada.
Little is known about the association between residence location and outcomes for chronic conditions, especially those that require lifelong supervision by a specialist, such as kidney failure. Although renal programs around the world deliver services to people who live in remote areas through the use of satellite hemodialysis units, few studies have examined how residence location affects clinical outcomes among patients receiving dialysis. A recent study showed that mortality was similar among US hemodialysis patients who lived in rural and urban areas.12 However, the authors of this study did not estimate distance or travel time to nephrology services. We used distance to define residence location, because although almost all remote communities are rural, the converse is not necessarily true.6 A previous study from our group found that the likelihood of receiving a kidney transplant in Canada is not influenced by residence location, which suggests that even complex processes can operate equitably for patients in both remote and urban areas.1
We found a higher risk of death among patients who lived in remote areas. It is possible that people who live in remote areas may be healthier than those who live in urban areas; however, this would have biased the results toward the null hypothesis (i.e., similar mortality among patients both areas). Although people who live in remote areas may have reduced access to both primary care physicians and specialists, adjustment for an accepted index of physician supply did not alter our findings.6 Therefore, we speculate that the excess mortality among patients in remote areas may be a result of less frequent contact with a nephrologist, as compared to patients who live in urban areas.
In Canada, patients receive hemodialysis either at in-centre units, which have a nephrologist on-site or nearby, or at satellite units, which are supervised by a nephrologist or a group of nephrologists who primarily work elsewhere. There are no data that document how frequently Canadian nephrologists physically attend to their satellite hemodialysis patients, although it is clear that wide variation exists. Although most hemodialysis patients in Canada who live in urban areas are seen at least weekly by a nephrologist, it is unlikely that such frequent contact is possible for patients who live more than 150 km from their nephrologist. The increased risk of death from infectious causes among patients in remote areas may indicate that serious infections are not managed quickly or appropriately in hemodialysis units where nephrologists do not frequently attend. Alternatively, patients who live in remote areas may be more likely than those in urban areas to receive venous dialysis catheters rather than arteriovenous fistulae because of lower access to vascular surgery services,13 which may predispose these patients to death from sepsis. We did not have data on the management of infections or vascular access type; thus, these suggestions are speculative. Regardless, our findings identify an opportunity to improve outcomes among patients receiving hemodialysis in remote areas.
Our study has several limitations. First, our classification of residence location was based on data at the time of dialysis initiation and it ignored the fact that some participants may have moved after starting dialysis. However, since few patients move farther from their nephrologist after starting hemodialysis, the true excess risk of death among patients in remote areas is probably greater than that suggested by our findings. Second, the validated methodology we used to calculate distance necessitates some approximations. Therefore, we categorized distance from the attending nephrologist into relatively broad categories, which reduces the risk of misclassification. The third limitation is that agreement between the cause of death obtained from death certificates and from dialysis registries is poor.14 However, a preliminary study found that the specificity of “death due to infection” reported to the Canadian Organ Replacement Register was 100% when registry data was compared with the results of an independent chart review.15 Fourth, although people in the general population who live in remote areas may have a slightly higher risk of death than those who live in urban areas, the magnitude of the increased risk is small (about 0.1 excess deaths per 100 person-years),16 which would not explain our findings. The fifth limitation is that we restricted our analyses to patients receiving hemodialysis. However, in a previous study we obtained similar results for patients receiving peritoneal dialysis,4 which makes selection bias unlikely. Finally, despite our best efforts at statistical adjustment, it is possible that residual confounding by unmeasured characteristics may have influenced our findings.
Future studies should compare markers of high-quality care for patients receiving hemodialysis in both urban and remote areas. Studies should focus on markers that are amenable to intervention, including the type of vascular access17 and the frequency of sit-down rounds.10 In addition, the increased use of telemedicine or partnerships between nephrologists and primary care physicians may facilitate closer follow-up of patients with kidney failure who live in remote areas.18
In conclusion, we found that the mortality associated with hemodialysis was greater among patients who lived farther from their attending nephrologist, as compared with those who lived closer. This was apparently owing to a higher likelihood of death from infectious causes. Our findings identify an opportunity to improve outcomes among patients receiving hemodialysis in remote areas through further studies and targeted interventions.
@ See related article page 1055
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/177/9/1039/DC1
This article has been peer reviewed.
Contributors: Marcello Tonelli conceived the study and wrote the first draft of the manuscript. All of the authors participated in the study design and statistical analyses. All of the authors critically revised the manuscript for important intellectual content and approved the final version for publication.
Acknowledgements: We thank Mr. Frank Ivis from the Canadian Organ Replacement Register for his assistance with data management.
Marcello Tonelli and Brenda Hemmelgarn are supported by Population Health Investigator Awards from the Alberta Heritage Foundation for Medical Research. They, along with Braden Manns, are supported by New Investigator Awards from the Canadian Institutes for Health Research and by a joint initiative between Alberta Health and Wellness, the University of Edmonton and the University of Calgary. John Gill is supported by the Michael Smith Foundation for Medical Research. This study was supported by operating grants from the Canadian Institutes for Health Research and the University of Alberta Hospital Foundation.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Clinicians perspectives on equity of access to dialysis and kidney transplantation for rural people in Australia: a semistructured interview study
- Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review
- Likelihood of coronary angiography among First Nations patients with acute myocardial infarction
- Geographic and facility-level variation in the use of peritoneal dialysis in Canada: a cohort study
- Hypoglycemia Associated With Hospitalization and Adverse Events in Older People: Population-based cohort study
- Adding Specialized Clinics for Remote-Dwellers with Chronic Kidney Disease: A Cost-Utility Analysis
- A Novel Technique to Optimize Facility Locations of New Nephrology Services for Remote Areas
- Adverse outcomes among Aboriginal patients receiving peritoneal dialysis
- Model for Equitable Care and Outcomes for Remote Full Care Hemodialysis Units
- A Comparison of Quality of Life and Travel-Related Factors between In-center and Satellite-Based Hemodialysis Patients
More in this TOC Section
Similar Articles
Collections

