


- © 2007 Canadian Medical Association or its licensors
What's your call?
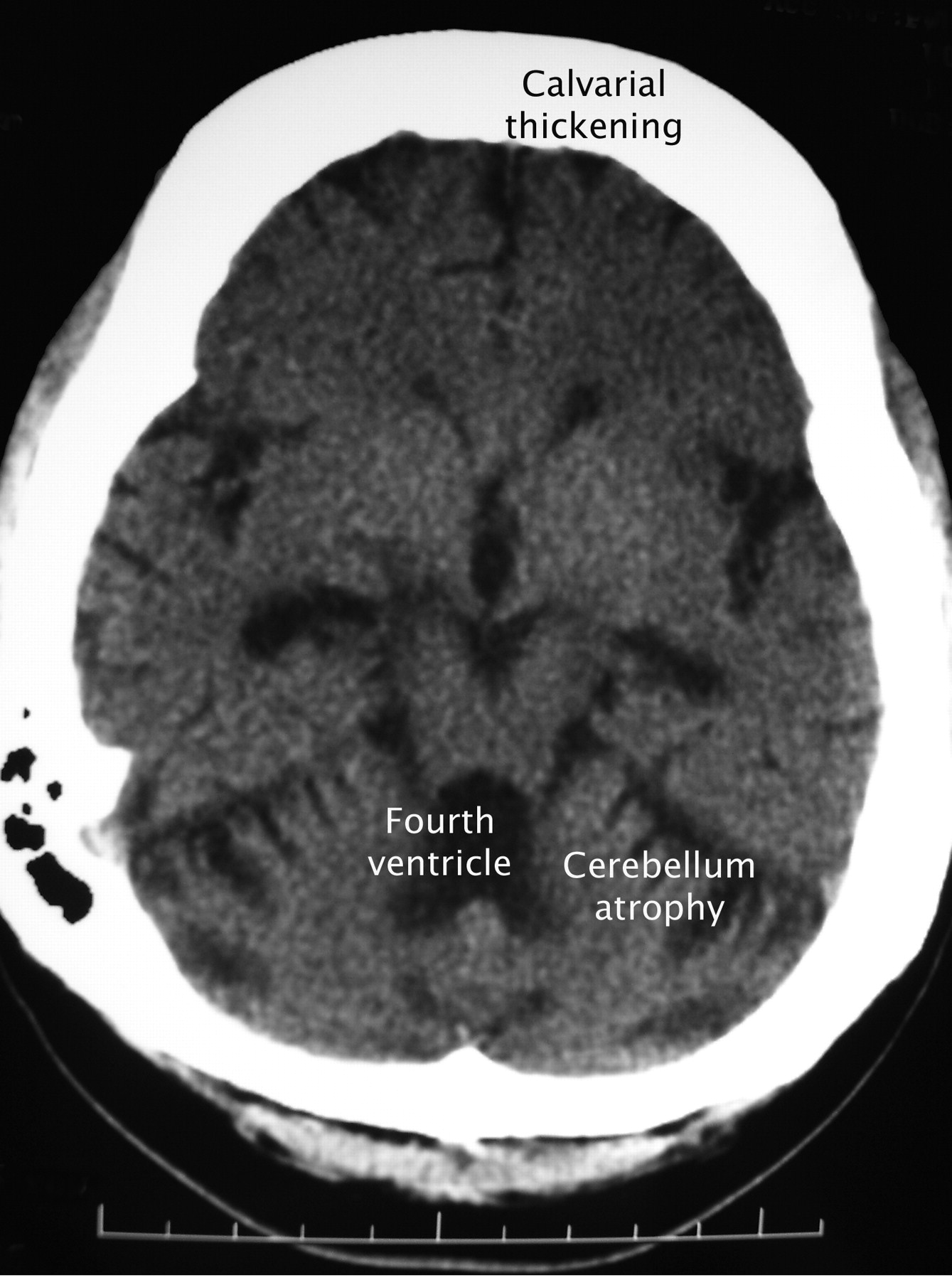
Figure. Axial plain CT scan of a 31-year-old woman with long-standing epilepsy who injured her head during a seizure.
The woman had refractory epilepsy and mental insufficiency since 15 years of age following an episode of encephalitis. Her epilepsy showed a fair response to adjunctive vagus nerve stimulation (placement of a bipolar electrode delivering intermittent electrical pulses to the left vagus nerve) in addition to chronic antiepileptic drug therapy (including phenytoin, sodium valproate, pregabalin and clobazam). The patient had been treated with phenytoin since the age of 18.
At age 31, the patient underwent a CT scan after experiencing a head injury during a seizure (Fig. 1). The result of the CT scan is remarkable because it demonstrates 2 distinct effects of chronic anticonvulsant therapy: cerebellar atrophy and generalized thickening of the skull vault. In this patient, cerebellar atrophy appears to have developed after the use of anticonvulsants rather than encephalitis. The chronological sequence makes post-encephalitis changes less likely, however this possibility cannot be completely excluded.

Fig. 1: Axial plain CT scan after prolonged anticonvulsant therapy showing cerebellar atrophy with secondary dilation of the fourth ventricle and marked (symmetrical) hyperostosis of the skull.
The adverse effects of phenytoin on skull thickening have long been recognized.1 Phenytoin has recently been shown to stimulate osteoblast proliferation and differentiation via upregulation of transforming growth factor-β1 and bone morphogenetic proteins. The exact incidence of calvarial thickening is unknown, but has been reported to be 34% among patients with seizure disorder in institutions.2 The clinical implications of skull thickening appear to be largely cosmetic: the degree of skull thickening correlates with frontal bossing (acromegaloid features with normal hand and foot size) and the degree of facial coarsening.
Other causes of bilateral hyperostosis of the skull vault, such as marrow hyperplasia secondary to thalassemia major, hyperparathyroidism, acromegaly and osteopetrosis, were not evident in this patient.
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

